Your new post is loading...

|
Scooped by
Juan Lama
|
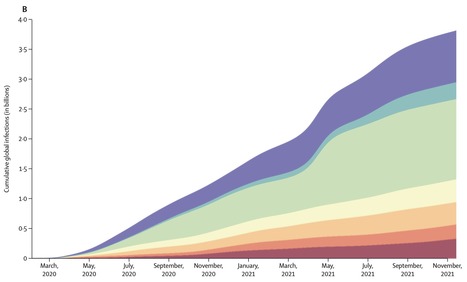
COVID-19 has already had a staggering impact on the world up to the beginning of the omicron (B.1.1.529) wave, with over 40% of the global population infected at least once by Nov 14, 2021. The vast differences in cumulative proportion of the population infected across locations could help policy makers identify the transmission-prevention strategies that have been most effective, as well as the populations at greatest risk for future infection. This information might also be useful for targeted transmission-prevention interventions, including vaccine prioritisation. Background Timely, accurate, and comprehensive estimates of SARS-CoV-2 daily infection rates, cumulative infections, the proportion of the population that has been infected at least once, and the effective reproductive number (Reffective) are essential for understanding the determinants of past infection, current transmission patterns, and a population's susceptibility to future infection with the same variant. Although several studies have estimated cumulative SARS-CoV-2 infections in select locations at specific points in time, all of these analyses have relied on biased data inputs that were not adequately corrected for. In this study, we aimed to provide a novel approach to estimating past SARS-CoV-2 daily infections, cumulative infections, and the proportion of the population infected, for 190 countries and territories from the start of the pandemic to Nov 14, 2021. This approach combines data from reported cases, reported deaths, excess deaths attributable to COVID-19, hospitalisations, and seroprevalence surveys to produce more robust estimates that minimise constituent biases. Methods We produced a comprehensive set of global and location-specific estimates of daily and cumulative SARS-CoV-2 infections through Nov 14, 2021, using data largely from Johns Hopkins University (Baltimore, MD, USA) and national databases for reported cases, hospital admissions, and reported deaths, as well as seroprevalence surveys identified through previous reviews, SeroTracker, and governmental organisations. We corrected these data for known biases such as lags in reporting, accounted for under-reporting of deaths by use of a statistical model of the proportion of excess mortality attributable to SARS-CoV-2, and adjusted seroprevalence surveys for waning antibody sensitivity, vaccinations, and reinfection from SARS-CoV-2 escape variants. We then created an empirical database of infection–detection ratios (IDRs), infection–hospitalisation ratios (IHRs), and infection–fatality ratios (IFRs). To estimate a complete time series for each location, we developed statistical models to predict the IDR, IHR, and IFR by location and day, testing a set of predictors justified through published systematic reviews. Next, we combined three series of estimates of daily infections (cases divided by IDR, hospitalisations divided by IHR, and deaths divided by IFR), into a more robust estimate of daily infections. We then used daily infections to estimate cumulative infections and the cumulative proportion of the population with one or more infections, and we then calculated posterior estimates of cumulative IDR, IHR, and IFR using cumulative infections and the corrected data on reported cases, hospitalisations, and deaths. Finally, we converted daily infections into a historical time series of Reffective by location and day based on assumptions of duration from infection to infectiousness and time an individual spent being infectious. For each of these quantities, we estimated a distribution based on an ensemble framework that captured uncertainty in data sources, model design, and parameter assumptions. Findings Global daily SARS-CoV-2 infections fluctuated between 3 million and 17 million new infections per day between April, 2020, and October, 2021, peaking in mid-April, 2021, primarily as a result of surges in India. Between the start of the pandemic and Nov 14, 2021, there were an estimated 3·80 billion (95% uncertainty interval 3·44–4·08) total SARS-CoV-2 infections and reinfections combined, and an estimated 3·39 billion (3·08–3·63) individuals, or 43·9% (39·9–46·9) of the global population, had been infected one or more times. 1·34 billion (1·20–1·49) of these infections occurred in south Asia, the highest among the seven super-regions, although the sub-Saharan Africa super-region had the highest infection rate (79·3 per 100 population [69·0–86·4]). The high-income super-region had the fewest infections (239 million [226–252]), and southeast Asia, east Asia, and Oceania had the lowest infection rate (13·0 per 100 population [8·4–17·7]). The cumulative proportion of the population ever infected varied greatly between countries and territories, with rates higher than 70% in 40 countries and lower than 20% in 39 countries. There was no discernible relationship between Reffective and total immunity, and even at total immunity levels of 80%, we observed no indication of an abrupt drop in Reffective, indicating that there is not a clear herd immunity threshold observed in the data. Published in The Lancet (April 8, 2022):
|
|
Scooped by
Juan Lama
|
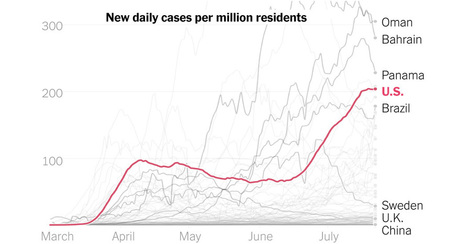
The United States is among the countries facing the worst of the global outbreak, while much of Europe and Asia has flattened the curve. This chart shows the countries with the worst coronavirus outbreaks in the world right now. With its cases surging since mid-June, the United States is squarely in the top 10. Leading the outbreak now are countries in the Persian Gulf, where the virus has spread rapidly among foreign laborers. Rounding out the top 10 are South Africa, Israel and several countries in Latin America. The current U.S. outbreak is especially stark when compared to other large, high-income countries. All have few cases today compared to the United States. South Korea had the earliest outbreak among these countries, but widespread testing and thorough contact tracing rapidly stopped the spread. South Korea now has the lowest infection rate of the group. Italy and Spain saw some of the worst early outbreaks, before strict control measures brought cases down. Now, some schools are open, adults are back at work and tourists are on vacation. Even Sweden, where cases surged after the government chose to forgo the strict lockdowns of its neighbors, has seen cases drop. The surge in the United States is so extreme that, once adjusted for population, these 10 states are recording more new cases than any country in the world.
|
|
Scooped by
Juan Lama
|
A new analysis reveals that more than 44% of new diagnoses are in people age 34 or younger, up from 29% a month ago. Only 30.5% are in people over age 50. As California’s economy opens up, coronavirus cases are getting younger and younger. An analysis released this week reveals that more than 44% of new diagnoses are in people age 34 or younger, up from 29% a month ago. There’s a corresponding drop in cases among older people. The proportion of COVID-19 cases among Californians older than 50 has plummeted from 46% to 30.5% in the past month. The proportion of cases among middle-aged Californians — ages 35 to 49 — has plateaued, neither rising nor falling. “It is striking that there is such a strong shift. Cases are much younger now than they were earlier in the pandemic,” said infectious disease epidemiologist George Lemp, who calculated the trends using historical data from the California Department of Public Health. “It may reflect the opening up of California since mid-May, particularly among younger people who may have started to move away from the practices of social distancing and consistent mask use,” he said. It’s unknown whether the shift is in part due to the increased availability of tests to everyone who wants one. California has significantly expanded its testing capacity — scaling up from just 2,000 per day in April to more than 60,000 tests per day this week. The state does not report overall trends in COVID-19 cases, by age. But Lemp recorded and archived the data from three different snapshots in time to detect the dramatic shift. People between ages of 18 to 34 now claim the largest share of new infections in the state, with 12,919 known cases diagnosed between May 31 to June 13. The second largest group, with 9,691 new cases, are people between the ages of 35 and 49. There has been a worrisome jump in youth under the age of 17. From the beginning of the pandemic until May 13, cases were rare, with a cumulative tally of only 2,799 diagnoses reported in this group. But that number was surpassed in merely two weeks, between May 14 and May 30, with 3,455 new cases. And it was exceeded again between May 31 and June 13, with 3,930 new cases....
|
|
|
Scooped by
Juan Lama
|
The COVID-19 infection rate among pregnant women was estimated to be 70% higher than in similarly aged adults in Washington state, according to a new study published today in American Journal of Obstetrics and Gynecology. Other key findings include: The study also showed that the number of COVID-19 infections in pregnant patients from nearly all communities of color in Washington was high. There was a twofold to fourfold higher prevalence of pregnant patients with COVID-19 infections from communities of color than expected based on the race-ethnicity distribution of pregnant women in Washington in 2018. A high number of pregnant women with COVID-19 received their medical care in a language other than English. This indicates that public health outreach to enhance vaccination rates in these communities is crucial. COVID-19 vaccine allocation is based priority lists set by each state's department of health, which can vary. In some states, pregnancy is considered a high-risk health condition for COVID-19 vaccine allocation in Phase 1B. Texas, New Hampshire, New Mexico and Alaska are among the states that prioritize pregnant women for COVID-19 vaccines in schedule Phase 1B. "The vaccine distribution plans vary quite a bit, state-by-state, and pregnant women are written out of the allocation prioritization in about half of U.S. States. Many states are not even linking their COVID-19 vaccine allocation plans with the high-risk medical conditions listed by the CDC - which include pregnancy, Adams Waldorf said. "The higher infection rates in pregnant patients, coupled with an elevated risk for severe illness and maternal mortality due to COVID-19, suggests that pregnancy should be considered a high-risk health condition for COVID-19 vaccine allocation in Phase 1B all across the United States," she added. "The time to act is now." She said this study is unique in the United States because it is the first to address the question of infection rates in pregnancy in a large population that represents the majority of pregnancies in the state. The data can inform vaccine policy and guide public health workers and physicians in trying to mitigate COVID-19 in vulnerable populations. The multisite study included 35 hospitals and clinics that compose the Washington State COVID-19 in Pregnancy Collaborative led by Adams Waldorf and Erica Lokken, an epidemiologist at the UW School of Public Health. The group identified 240 pregnant women who acquired COVID-19 from March through June 2020. This number represents all such known cases at the collaborating sites, which account for 61% of births in the state each year. "Higher infection rates in pregnant patients may be due to the overrepresentation of women in many professions and industries considered essential during the COVID-19 pandemic - including healthcare, education, service sectors," said Lokken. Pregnant women may also have larger households, children in daycare or playgroups, and be caregivers within an extended family, she added. This study data fills critical gaps and provides an important estimate of regional COVID-19 infection rates in the pregnant population, Waldorf said. The Centers for Disease Control and Prevention's estimated infection rates may not be representative, she said. "COVID-19 case reports are missing pregnancy status in up to 65% of reports for women of reproductive age. As a result, the number of pregnant patients infected with COVID-19 was likely underrepresented in national numbers," the authors concluded. "When the data is woefully incomplete for specific groups, like pregnant women, it is easy to assume that they haven't been impacted by the pandemic. This was not the case," said Adams Waldorf. Pregnant healthcare workers have received the COVID-19 vaccine, and Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, has reported no "red flags" in preliminary data about post-vaccination well-being of this population. Adams Waldorf urges pregnant women to discuss the risks and benefits of COVID-19 vaccination with their prenatal care provider. More ob-gyns have begun recommending that pregnant women take the vaccine. "We want to use information from this study to be more prepared for the next pandemic and to not brush pregnant women to the side. They need to have a seat at the table when it comes to vaccine trials and vaccine allocation," Adams Waldorf said. American Journal of Obstetrics and Gynecology (Feb. 9, 2021): https://doi.org/10.1016/j.ajog.2021.02.011
|
|
Scooped by
Juan Lama
|
Scientists say samples from Milan and Turin showed virus traces long before cases were confirmed. Italian scientists say sewage water from two cities contained coronavirus traces in December, long before the country's first confirmed cases. The National Institute of Health (ISS) said water from Milan and Turin showed genetic virus traces on 18 December. It adds to evidence from other countries that the virus may have been circulating much earlier than thought. Chinese officials confirmed the first cases at the end of December. Italy's first case was in mid-February. In May French scientists said tests on samples showed a patient treated for suspected pneumonia near Paris on 27 December actually had the coronavirus. Meanwhile in Spain a study found virus traces in waste water collected in mid-January in Barcelona, some 40 days before the first local case was discovered. In their study, ISS scientists examined 40 sewage samples collected from wastewater treatment plants in northern Italy between last October and February. Samples from October and November came back negative, showing that the virus had not yet arrived, ISS water quality expert Giuseppina La Rosa said. Waste water from Bologna began showing traces of the virus in January. The findings could help scientists understand how the virus began spreading in Italy, Ms La Rosa said. However she said the research did not "automatically imply that the main transmission chains that led to the development of the epidemic in our country originated from these very first cases". Italy's first known non-imported virus case was a patient in the town of Codogno in the Lombardy region. The town was closed off and declared a "red zone" on 21 February. Nine other towns in Lombardy and neighbouring Veneto followed and the entire country went into lockdown in early March....
|